It’s been 5 months today since my surgery and it’s looking like the surgery was a big mistake, as I expected it would be. The past week has been particularly miserable. I really wish I could just die. The reality is, I’m probably stuck with this pain for the rest of my life. I’d like to at least know what’s causing it.
I was originally diagnosed with Facet Joint Syndrome. I think I need to find doctors and approach it from that perspective.
These aren’t just dark times. I’m terrified! If the old pain continues to worsen I’m going to have two choices – suicide or medication. Medication would probably work except this country has decided to stop medicating pain patients. A small dose of methadone can relieve a tremendous amount of suffering but because it falls under the class “opiate”, pain patients are now caught up in DEA’s War on Drugs. So what happens? Doctors ignore their hippocratic oath and let us suffer, refusing to prescribe pain medication to pain patients. These patients will suffer until they can’t take it anymore so they commit suicide or go out on the streets or the Dark Web for medication. If things don’t improve soon, I’m going to have to start looking for a doctor willing to increase my dose of methadone to what the UCSF pain clinic recommended, 30mg/day. I may need to leave the country. Part of me really just wants to end it all. I’ve suffered more pain than any animal should be forced to suffer. At 65, my life is pretty much over anyway, especially if I have to live the rest of it in horrible pain, on top of all the aches, pains, restrictions and illness of old age. Is it really worth it? I could say I should stay alive for Barbara but I’m not sure I’m doing her any favors. I’m basically a burden. I can’t take care of myself. I’m probably just preventing her from living a good life.
I suppose I might be depressed. I don’t want to get out of bed. I could say that it hurts more when I get out of bed but I’m not sure that’s even true. I’m determined to start walking at least 1 mile a day. I’ve been living with Level 7-8 pain every day. I suppose the surgical pain is getting better. I’d say it’s about level 7 so while it’s not any worse than the old pain, it’s probably adding to it. I still have slim hope that as the surgical pain settles down, so will the back pain. It does kinda feel like they both involve the same nerves. What I need to do is turn my brain off because worry rarely helps anything. In fact it can be my worst enemy. I need to try and not worry about anything. I do have my 5 week follow-up meeting with Dr. Hansen next week. I need to do some research to prepare for that.
I’m going to try to start walking down to the village for lunch every day at 11pm. I’ll my alarm for 9am, do tea and toast in bed, watch TV until 11, then walk. If I can do that every day, it will be a good sign. I think I’ll go ahead and buy a Sprinter. I have to create a life outside of this bed and getting back to nature has always been good for me. I’m sure there are a lot of trout to be caught in California, even if I can’t windsurf, snowboard, eFoil, surf or all the other things I want to do. Hopefully I’ll even be able to do those things next year. Trying to think positive and not kick myself for getting this surgery. I need to suck it up and be brave. Lately I’ve been thinking a lot about suicide. Hopefully it won’t come to that. Which reminds me, it’s time to sit down with Dr. Laurencin.
I can’t dwell on whether or not I should have gotten the surgery. I did and I need to move on. The next three months will be about healing. I can’t do much. I’ve been told not to bend, twist or lift over 15 lbs for 4 months. That’s pretty limiting. So I’m trying to walk twice a day for at least two miles. So far I’ve only been doing one mile walks every 2 or 3 days. That’s not good enough. I have recently added dumbbell exercises – curls and military press. My surgical pain is just slightly annoying, maybe pain level 3. The old pain (mid-back) is pretty much the same at PL 7-8.
Assuming this surgery was another red herring, I think the next step is an MRI and probably a PET-CT (PET for diagnostic purposes, CT to check on repair structure). To get this, I think I need to find a “spine doctor”, an orthopedic surgeon or a physiatrist. It may be time to resume looking for that needle in the medical haystack. Maybe I’ll start with California Orthopedic. They have a lot of orthopedic surgeons and physiatrists. I need to find a doctor that is interested in a challenge and willing to work with me. You’d be surprised how hard that is to find in a doctor. I just want some imaging and maybe some diagnostic injections.
The other thing I should probably do is explore the idea of rectus trigger points. I should be able to explore that on my own and when healed, make an appointment with Dr. Sawyer. For now, I need to shut down my negative thinking and come up with next steps in my search for a diagnosis. I should make an appointment with Dr. Salahuddin. I should check forums for radiology places. It’s too bad we can’t make appointments with radiologists. I need to drink more water and eat better, meditate and resume projects like guitar and robotics. Most of all, I need to try to enjoy life. Hopefully it will all be over soon.
OK, I went ahead and got the surgery and as I expected, I’m regretting it. I’ve let them make structural changes to my body that comprised the integrity of my ribcage permanently and I don’t think it addressed my problem. I think I had/have slipped ribs but not Slipping Rib Syndrome (slipped ribs causing pain). I.E. I think my costal cartilage on the left is the same as on the right – asymptomatic. I slept till 2pm today but when I woke the old pain was back. It started coming back yesterday. It’s probably just that my surgical pain is getting less so the old pain is once again the loudest barking dog (to use Dr. Hansen’s relative pain metaphor). I’m afraid it’s turning out just as I feared. I’ve not only added another physical problem to my list but now I’m essentially bedridden for the next 4 months to a year, going through various phases of pain, all for nothing!
So if SRS isn’t my problem, I need to go back to my list of suspects. They are, in order of likelihood…
Herniated left rectus abdominis, active for almost 20 years and requiring two surgeries. This is something my doctors all dismissed but that’s because most doctors are idiots and pretty much all available doctors are available for a reason. My core wreck is the only thing differentiating my left side from my right. The pain seems to radiate from the ab to the mid-back. This is common with rectus abdominis trigger points. I need to continue trigger point release, possibly with a trigger point expert. Perhaps I should consider getting the mesh removed. Unfortunately I’m approaching an age where people stop caring. However they never cared in the first place so I have to be my own doctor and use practitioners as tools. Anyway, the old 25 year old hernia is now my prime suspect.
Why is my vertebral marrow glowing? Osteitis, possibly from an autoimmune illness. In a PET scan, the vertebral marrow of my lower thoracic spine lit up like a christmas tree, with the left costotransverse/costovertebral joints as the lights. The Stanford (experimental) radiologist was sure the lit up vertebral marrow was a pain generator. He said it is seen in patients with long-standing autoimmune illnesses. This is especially interesting because I was diagnosed with PMR, then RA, then GCA, a few years ago but the pain started a decade before that. So if the pain is from an autoimmune illness, I suspect it’s one that started around 2009 or 2010. I remember feeling bad in the evenings. I was drinking too much and not taking care of myself. I need to research active vertebral marrow in PET scans. I am going to make an appointment with my old local rheumatologist (Dr. Dietz doesn’t seem open to experimental results but Dr. Biswald seems like a trustworthy source to me. But why is the pain unilateral? I think my next step here is to make an appointment with Dr. Ramanujam.
GI issue. There is definitely a GI connection. I can set off The Pain by drinking too much coffee or something spicy. The angry nerve has a branch into my stomach. While a GI problem may not be the root cause of the problem, it is definitely involved and should be considered a potential prime suspect.
Facet Joint Syndrome/Volleyball accident – This was my original diagnosis 15 years ago from Dr. Schofferman. I think I damaged the facet joint at LT10/11 in the mid-nineties. It was sore for years, then went away however if memory serves, it felt very similar to The Pain. Perhaps it is an old injury come back to haunt me. I don’t know if it’s primarily a muscle, joint or nerve problem and the pain syndrome that I have developed over time may be different from the original problem but I don’t think so. I think it may be as simple as an arthritic facet joint.
Dark Times
I wake up in the mornings terrified. I’ve been tortured for 15 years and I can’t find a doctor that will give me (my condition), the time of day. At this point I just want it to end. I haven’t given up on the Slipping Rib Surgery completely just yet but I think that’s just a matter of time before I realize that it did nothing to address my pain, it just created new issues. I’ve lost all faith in doctors. If there were a button that would end this torture (i.e. my life) I probably would have pressed it by now. It’s not that easy to kill yourself. It’s a violation of the prime objective – survival. But a life is not worth living if it is lived above a certain pain level. We euthanize other animals, why not ourselves. I don’t want to drag this out forever. Everyone will think it’s depression and maybe they’ll be right, but most people have no idea what it’s like to live with severe chronic pain. They just can’t (or choose not to) wrap their heads around it. Empathy does not come easily to the human animal. I’m trying to be positive and heal from the surgery. This surgery is nothing like the other 5 or 6 surgeries I’ve had over the years. The recovery is long and painful and my activity is very limited. Perhaps it’s good that I’m depressed and just want to sleep all day. I won’t really know if works for up to a year. I do know I’m still in too much pain to reduce my methadone. Even 1/2 mg/day change is very noticeable and as I learned at Stanford, “pain begets pain”.
Next Steps
Make appointment with Dr. Ramanujam
Find a good osteopath
Look into getting a PET/CT scan
Experiment with stomach meds during flare-ups (drink more water)
Research active vertebral marrow and pain that radiates to the back (from abdominal trigger points, GI, etc)
I’ll probably be rapid-cycling on the decision to have this surgery right up until they put me under. My confidence that this is a good idea is down to 20%. I truly believe I will regret it. The main reasons I have to doubt SRS as the source of “The Pain” are:
If it’s an intercostal nerve, I’ve narrowed it down to the 10th one. However a slipped 9th rib should be irritating by 8th intercostal nerve. I have no pain at T8/9.
My right side is almost identical to the left (both have floating 10th ribs and slipped 9th). Ok, so the left side is slightly more slipped but still, my cartilage configuration is not giving me any issues on the right. I have a lot more going on in the left that has nothing to do with slipped ribs like…
A wrecked left core, especially the rectus abdominis. My hernia, twice repaired has wreaked havoc on my left core, maligning and realigning muscles and joints. However there has been a study about a link between SRS and a weak left ab. So it’s possible my hernia is combining with hypermobile ribs to cause The Pain. I’m just not sure reconstructing my costal cartilage is going to address the back pain.
The surgery is brutal with discouraging results. It is only 50% successful, meaning they have to go back in and fix the repair about half the time. The average pain reduction after 1 year is only 50% and that’s after a year of extreme pain in some cases. At least 5 patients want their 3.0 reconstruction ripped out.
I’ve read way more failure stories than success stories. This is partly because people that are still hurting tend to be online while the people that are feeling good are out having fun but still, I’d expect to see more positive results. I’m disappointed with myself that I didn’t research more.
There’s a good change that this procedure will increase my pain long term, certainly short term.
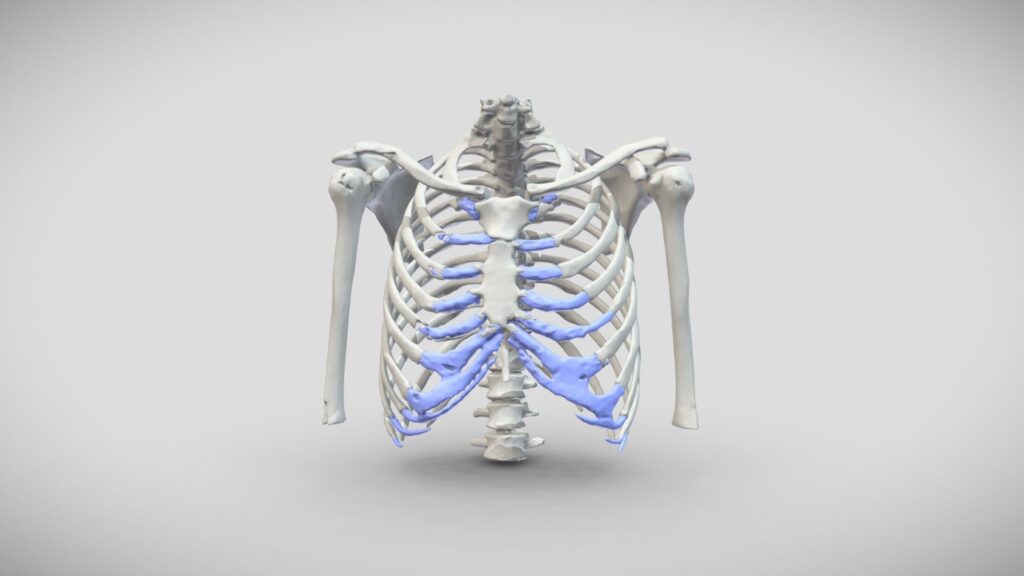
The photo above is from a “normal chest”. There is new information that we don’t have the perfect two floating and three false ribs like we were told. In fact I’ve been reading that most of us, up to 60% has 3 floating ribs, like me. Also, many people have subluxed ribs, can click them with the hooking maneuver, yet have no pain. Even Dr. Hansen has this. I can’t help thinking that if all this (pain from these ribs) were “real” it wouldn’t be so “rare”.
Here are some reasons to go ahead and get the surgery:
I’m desperate. If it works, the payoff is huge. Unfortunately it’s not like an injections where if it doesn’t work, no harm done. My ribs and life will probably never be the same and certainly not for a month to a year.
If I don’t try it, we’ll never know. ’nuff said. Everyone will think I’m crazy (or a pussy) not to get this surgery)
Dr. Hansen “feels strongly” that he can reduce my pain by at least 50%. Dr. Paul says I definitely have Slipping Rib Syndrome and hypermobile ribs. He confirmed tender to touch on palpation at the hypermobile ribs.
There is a plethora of symptoms associated with this syndrome. I should be trying to second-guess the experts at this point. I’ve become so skeptical of what doctors tell me. I just don’t trust them. Hopefully I can trust Drs. Paul and Hansen. I like both of them. They are by the way, the only two doctors I have seen, out of about 40-50, that have ever heard of Slipping Rib Syndrome. It’s been around for over a century and it’s more underdiagnosed than rare. There are a lot of reason for this ignorance but they add up to a broken medical system which is what we have in this country. Ask any chronic pain person.
Barbara has a 50% confidence rate. We’re both skeptics. I owe it to her to try anything and everything.
No doctor or practitioner has been able to figure out why my left rib cage always appears swollen. As if the muscles are inflamed. SRS is one of the few things that would explain this.
Floating 10th ribs can be symptomatic. I think that if I do have SRS, it is from my floating 10th rib, not my slipped 9th.
As you can see, it’s pretty evenly balanced. I travel in two days and the surgery will be two days after that. So I have 4 days to chicken out. Unless I can convince Barbara that I shouldn’t be doing this. I guess I’ll be going under the knife.
I’ll probably get the surgery. Regardless, I need to work on my attitude. I have been dragging Barbara down with me and I need to figure out how to be more pleasant. It’s true what they say “Pain is selfish”!
Dr. Paul’s diagnosis: “general palpable unstable T eight,nine and T9 T10 articulation, That is tendered Touch (some typos here). he also has tenderness in the T 9, T10 and to illustrate T11 costotransverse regions.” and “Impression/ plan #1instability, of the T8 and T9 articulation front and back, T9 and T10 significantly in the front. “. This is a YES vote because he notes tenderness at T8/9 as well as the costotransverse regions. However, one thing that worries me is that we had the range narrowed down to T10-T11, not T8-10.
Barbara – she is less skeptical than I am but she’s not as concerned with the surgery ending my active life. I’m afraid that “The Pain” is not from my slipping ribs. My right side is almost identical to my left (floating 10th ribs and slipped 9ths) but is asymptomatic. I worry that The Pain is from Facet Joint Syndrome, my wrecked left ab/core or possibly even an autoimmune disease. The vertebral marrow shows high uptake that the radiologist who specializes in radiology for pain at Stanford, feels is a significant pain generator. If I had more typical symptoms of SRS, like pain at T8/9 near the spine and pain at the subluxated rib tips, I’d be more confident in the diagnosis.
I was pretty honest with Dr. Hansen about level 8 being too high as well as most of my pain being near the spine and he seemed fairly convinced. AI (that’s my nickname for anything I’ve found on the web) says that a floating 10th rib alone is considered a version of Slipping Rib Syndrome. That means 60% of us have it! Both AI and Dr. Hansen said a congenitally floating 10th rib can be symptomatic.
One of the Dr. Hansen’s patients in my favorite knife/spear video does’t claim to have much pain at his rib tips, more tightness. I’m not really sure where his pain was because he said his back was tight too but this is the video where Dr. Hansen points out the knife in the back and spear through the body to the costal arch and up to the xiphoid which was the biggest selling point for SRS for me.
Stomach problems and digestive issues are symptoms of SRS, not FJS
Everyone as noted that my left back looks bigger than my right back. Visible inflammation is a symptom of SRS, not FJS
Fuck it – we need to rule everything out. There’s no good fix for FJS so let’s hope it’s SRS.
NO
Pain has been thought to be from T9-12, actually my left T10/11 facet joint is my best guess. A facet injection at 9/10 felt too high. Maybe I shouldn’t let these levels bother me too much but I don’t have pain at T8 – the location that a subluxed 9th rib should affect. That’s two levels too high! A floating 10th rib can be symptomatic but still, I don’t have pain at the expected places. The original diagnosis was facet arthropathy at T10-12. This correlates more with the levels of my back pain. Dr. O’Neill believed the facet joints to be only part of the problem based on “mixed results” from the ablation. However it all comes down to how I said it made me feel. If I remember correctly, it successfully addressed the spine pain but created more flank and superficial pain (I think it irritated the intercostal nerves. So why did we abandon the facet joint theory so quickly and permanently years ago? I think that was a mistake.
I seem to get a momentary feeling of muscle tearing or nerve being hit when I bend backwards too far, right at the spot where The Pain is. It seems to be hitting The Nerve, but the only way I can recreate this is with a back bend, again suggestive of Facet Joint Syndrome
I don’t have a lot of pain at the subluxated rib tips. This is the one symptom that even Dr. Hansen says, if there is no local pain at the rib tips it makes him question the diagnosis.
I just feel The Pain is from nerve impingement at T10/11, probably one of those three joints that hang together (costotransverse, costovertebral and facet). That would kind of rule out Slipping Rib Syndrome as a pain generator. Now if that’s something I’m willing to do at the cost of being much less active the rest of my life, fine. I’m just not there yet. 🙁
Procedure: Left T10-11 (T11) and left T11-12 (T12) medial branch nerve block
“Patient had undergone previous Medial Branch Block at T9,10 but felt injection was too high/”low” despite radiographic evidence. “Dr. Schofferman has recommended Medial Branch Block T10-11 and T11-12”
MRI T-Spine wo Contrast (7/9/2012)
Chronic Mild Schmorl’s nodes are present at T9 and T11. Mild disk height loss at T9-10. Mild to moderate facet arthropathy from T9-10 to T11-12 without significant foraminal narrowing.
Facet Rhizotomy January 2012 Dr. Gamburd
mixed results, some improvement for a few months
O’Neill Initial Assessment 12/10/2012
“Mild tenderness to palpation at approx T10/11” (2013 followup notes tenderness to palpation at T9/10). Imaging shows mild degenerative disease at T9/12 and facet arthropathy at T9/10, T10/11, T11/12.
“Partial response to rhizotomy indicates facet joints may be part of the problem but not the whole problem. Costovertebral and costotransverse joints may be a source of pain. Another possibility is nerve root irritation from the lateral recess compromise.”
Selective Nerve Root Injections (2/26/2013)
Left T9/10, T10/11 and T11/12
Followups: “Those definitely helped him, although for not more than a few weeks”. “Greg has chronic thoracic pain that is probably mechanical, although there could be a neuropathic component.”
“It seems we have zeroed in on the source of Greg’s pain which is in the thoracic spine somewhere between T10 and T12 on the left.” “Given the definite but partial benefit with selective nerve root injections, repeat nerve root injections could be helpful. The other option would be to inject the joints between the ribs and the vertebrae which have not been treated before.
Costovertebral Joint Injections Left T10,11,12 (12/23/2013)
(no followup but from what I remember these weren’t especially helpful)
My Impressions:
““Partial response to rhizotomy indicates facet joints may be part of the problem but not the whole problem. Costovertebral and costotransverse joints may be a source of pain. Another possibility is nerve root irritation from the lateral recess compromise.”
I think this is when we got away from the facet joints. Why we never came back to them is beyond me! Probably that blotched ablation. It hurts when they fry the wrong nerves, especially when they just partially fry them around your whole body. Oh well, it would suck to get ablations every couple of years. Those fucking nerves grow back. I’m just not sure nerve frying is the solution to anything. I suppose they need some desperation options other than opiates. Maybe I just got a bad one. Oh well, that will probably be my next Hail Mary if this Hansen 3.0 doesn’t work.
All of this T9 – 12 stuff has me worried though. I’m supposed to be hurting at T8. He (as well as AI) said that I could have symptoms from my hypermobile 10th rib, even though it’s congenital and thus I suppose, my 9th. It would explain why I don’t have pain at my 9th rib tips. It would all makes sense if The Pain and those blobs were at level 8 and not level 10. But what if my ribs are the problem? I mean, they’ve been jerked and pulled around by my sports, my hernia, the 2nd surgery. Like this article says, there’s a lot moving around in there when your 10th rib is floating.
Dr. Rowan Paul’s Office Visit
Office Visit Note
Patient Name: Gregory Payne
D.O.B.: 08/01/1960; 64 yrs, 7 mo at the time of visit
Seen by Rowan Paul, M.D.
Date: 03/05/2025
Exam Reason (CC): SF MSK EST FU
History of Present Illness
Gregory is a 64 year old man here for left lower rib pain. Feels like his pain was posterior but more unstable. Sharp knife in the back, then flank ache and has had negative rib fractures. 9./10 in the morning, has to take Methadone, Cymbalta. 4-6/10 now.
Cortisone injections was helkpful for 4 hours from the anesthetics. Steroids didn’t work.
Weakened abdominal muscles. History of diastasis recti.
Bone scan remotely was negative.
Is going to see Dr. Hansen in West Virgina for Hansen technique
Otherwise as seen in the common Electronic health record, no change in past medical history, past social history, family history, medications, allergies
ROS:
CONSTITUTIONAL: Appetite good, no fevers, night sweats or unintentional weight loss. HEENT: No headaches, diplopia, eye pain, ear pain, tinnitus, nose bleeding, mouth sores, or jaw claudication. CV: No chest pain, shortness of breath, dyspnea of exertion, or peripheral edema. RESPIRATORY: No cough, wheezing, or dyspnea. GI: No nausea/vomiting, diarrhea, abdominal pain, or change in bowel habits. GU: No dysuria, urgency, or incontinence. NEURO: No motor weakness or sensory changes SKIN: No rash or photosensitivity. MUSCLE-SKELETAL: No morning stiffness, Raynaud’s Phenomena, Positive joint pain/ muscle/tendon pain as above ENDOCRINE: No polyuria/polydipsia, no heat or cold intolerance
on exam the patient is in no apparent distress Psych: alert and oriented, lungs with non-labored breathing, no audible wheezing or tachypnea. Neck is supple, trachea midline. Extremities are warm and well-perfused, no clubbing cyanosis or edema. Heart regular rate and rhythm,no varicosities Skin with no visible skin lesions or lacerations. no erythema. Neurovascularly grossly intact with full motor and sensory function besidesbelow. DTR 2+ bilaterally Patellar and Achilles, nonantalgic gait MSK: general palpable unstable T eight,nine and T9 T10 articulation, That is tendered Touch. he also has tenderness in the T 9, T10 and to illustrate T11 costotransverse regions.
Completes nonvascular real time ultrasound examination clearly shows instability, of the T8 and T9 articulation front and back, T9 and T10 significantly in the front. I do not see major instability at T10 T11 though he does have pain under the ultrasound probe. underlying lung looks intact.
Impression/ plan #1instability, of the T8 and T9 articulation front and back, T9 and T10 significantly in the front. Likely post traumatic in the setting of Ehlers Danlos syndrome.
I recommend a dextrose based prolotherapy And Shockwave therapy as well as Class for high potency robotic assisted laser and EMT. he and his wife were minimal after risks and benefits were explained. I recommend to treating both Anchor and posteriorly based on his biomechanics. He could opt to do surgical stabilization as well.
Was crept with chlorhexidine times three. under direct needle ultrasound guidance with image documentation using a sterile 6 to 15 megahertz ultenrobe by advanced at 25GAGE needle in long axes and then short axes and injected the T8T9 and T10 cost of transverse joints posteriorly. I then injected the anterior slipping rib at T8, T9 and T10 with 4ml of 12.5 % dextrose, 2 ml of 0.2% ropivicaine.
MLS Class 4 laser neuritis setting front and back.
The patient tolerated the procedure well, no complications. Lungs CTA bilaterally after. Felt much better after. No pain.
See back in 6 weeks.
Patient was advised to seek urgent medical care if they develop any sudden worsening pain, weakness, parasthesias, bowel or bladder incontinence, saddle anesthesia, headache, fever, or chills. Medication precautions given. Conservative measures explained in detail. Activity modification discussed in detail Patient is amenable to treatment plan. Questions were answered. healthy lifestyle explained. Thank you for the opportunity to take care of this patient.
Assessment/Plan
1. Slipping rib syndrome
2. Thoracic back pain
3. Fascial defect
4. Abdominal pain
Electronically signed by Rowan Paul, M.D. on 03/05/2025 1:09 pm in .
I was reminded today that coffee sets off “The Pain”. It’s like pouring salt on a wound except it’s pouring coffee onto the nerves in my back that hurt. “The Internet” (maybe I’ll just start calling anything from the WWW, if that’s still a thing, AI). Anyway, AI says (hey I like that term, search results are intelligence and they’re artificial! Bingo! “AI” it is, to describe any rubbish I get from my browser.
OK, sorry, back to the point of this phenomenon supporting YES on the surgery in that, SRS is known for stomach issues, Facet Joint Syndrome, (FJS, my latest theory and first excuse for backing out of my upcoming surgery), is not. but here comes a bunch of NOs…
Facet Joint Syndrome
I was originally diagnosed with Facet Joint Syndrome. I even had an ablation which may have worked but it I think it was aimed wrong, creating new and different pain. I remember my left side swelling up like a football when the ablation was over. I want to say that it did relieve my primary pain for a couple of years but I can’t be sure. At any rate, the ablation was a bad experience and for some reason, I never went back to that diagnosis. Neither did the doctors.
PET scans have detected rib joint reuptake on the left>right but no facet joint issues. Oops, there’s a big YES. I can bend backwards a long way (YES) but I do reach a point that seems to send a jolt through The Pain (NO!). This is what makes me wonder the most. But that whole area (the three joints) is bound to be inflamed and I’m sure there are limits to the others as well, they are just more protected from stupid human moves. One of the ways they are protected (the rib joints) is from their ribs’ third connection in the front, which most ribs have. Now we know we’ve been lied to our whole lives. Did you know most people have 6 floating ribs? That’s right! Most of us have three floating ribs per side, not two! Now they’re telling is it’s about half and half and three has a slight (percentage or two, or three) edge. From pictures like the one at the top, Slipping Rib Syndrome is also just a variation of the norm. They are saying that is from a “Normal Chest”! So I have two congenitally floating 10th ribs and 2 subluxated 9th ribs (the left is more so). Both my sides click the same. However I only have symptoms on one the left? Why? Apparently this “condition” is often bilateral but with unilateral pain. Perhaps my hernia made them symptomatic, or that girl who walked on my back. But that volleyball incident was a hyperextension of my spine and haunted me for years. If my memory is correct, it was the same but lighter version of my current pain (The Pain). This equates to a big NO! It says that my problem is not SRS but FJS!
So we have one YES from the coffee trigger and a couple of NOs from SRS’s nimesis, FJS. We’ve discovered that I have floating 10th ribs and my ninth ribs are subluxated up under my 8th ribs, which should be irritating my eighth intercostal nerve but it’s NOt. My pain is from the 10th rib area (maybe 9th or 11th but not 8th!). So NO! But none of this really matters. I think I have to get this surgery for a couple of reasons….
Barbara
She has been a proponent of this surgery and theory the whole way. I’m much more skeptical. I’m giving it a 30/70 chance of making things significantly better but I have to do it for Barbara. It’s actually considered “minimally invasive” but I think it was Dr. Laurencin or somebody that said only a thoracic surgeon would consider it minimally invasive. I’m freaking out because Dr. Hansen basically told me it was the end of my active life, at least doing the sports I like to do. He pointed out that it should probably be that way anyway and I suppose he’s right. I was talking to Babs about it being an addiction and how it keeps me from enjoying the little things. I’m always chasing the dragon, wanting to be on the water or the trail, not in the moment. So whether this works or not, Barbara wants this surgery and ultimately I think it will be good for me to let go of my active life and pay more attention to her, enjoy the little things with her. Sigh… well at least this makes the decision easier.
Time to Break Out the Big Guns
I just turned 65 and my life is shit. I’m a miserable asshole who’s making everyone else’s life shit. Even if this is the red herring I think it is, it really won’t make things much worse. So there’s everything to gain and not really that much to lose. I keep hoping for a miracle cure that just isn’t coming. If this doesn’t work, I’ll turn our attention back to the facet joint. Fuck I really wish I could get a facet joint injection before the surgery.
This is driving me nuts. One minute I’m ok with the surgery, the next minute I’m convinced it’s a red herring. It’s just such a damaging red herring if it is. Here’s a quote from a paper about a swimmer that I keep running across…
Rib hypermobility caused by weakness of the rib-sternum (sternocostal), rib-cartilage (costochondral), and/or rib-vertebral (costovertebral/costotransverse) ligaments, allowing rib hypermobility, is thought to be the primary cause of slipping rib syndrome. Ribs 8 through 10 (false ribs), which are not connected to the sternum but are connected to each other via a cartilaginous cap or fibrous band, tend to be the most mobile and susceptible to trauma. Because of this, slipping rib syndrome is usually caused by hypermobility of rib 8, 9, or 10. Anterior rib hypermobility is also likely to cause problems in the posterior thoracic area as well because in a closed system (in this case, the rib cage) it is difficult for motion to occur at 1 site (the anterior portion of the rib) without causing motion to occur elsewhere (the posterior portion of the rib). So, as was the case with our athlete, the condition often results in back pain.
I guess I’m suspecting facet joint syndrome although I don’t really have the symptoms of that. I just have this gut feeling (pardon the pun), that reconstructing my costal margin is NOT going to make my back pain better. Now I’m learning that all this shit about having two floating ribs is bullshit. Turns out most of us have three! Apparently I have three floating ribs and my ninth rib is subluxated. This should be irritating my 8th intercostal nerve. That’s just to high! Perhaps it’s not the intercostal nerve at all but hypermobile ribs irritating muscle. They talk about the “closed loop” as mentioned above. If my 10th rib is causing the pain, perhaps it’s because I lack stabilizing cartilage in my 10th rib (a variation of normal).
OK, so hold on. Dr. Hansen said that the 10th rib can be problematic even when it’s congenital and there’s a lot online to support that. I was just thinking that my whole ribcage seems inflamed. Some even consider a floating 10th rib to be a version of Slipping Rib Syndrome. Bottom line is, it’s worth a shot, even though I don’t think it’s going to help. Time is running out and I’m getting desperate.
I was looking back at old journals today. There was a lot of mention of flank and rib pain as well as stomach pain. In fact I was blaming it on the stomach for awhile. They say stomach problems are very common with SRS.
I saw Dr. Hansen last week and he happened to have an appointment available on September 17th for surgery so I signed up. Now I’m freaking out. I’m just not 100% convinced that my back pain is from my slipped/hypermobile ribs/broken costal cartilage! In other words, I do have slipped ribs, I’m just not sure I have Slipping Rib Syndrome (pain from slipped ribs). Lots of peoples ribs click, including Dr. Hansen’s, but they don’t have pain. I have plenty of other physical issues on the left side of my body to cause back pain and I don’t have much pain at the subluxated rib tips (an important though not required symptom).
So I figure I have this week to decide. I can’t cancel any later than Friday. I’ll start with the things Barbara suggested:
Recently, it was discovered that I have a large blob of pain on my left mid-back, between the muscles and the skin. It has been described as spongy, like fluid, squishy. It’s very visible and baffles everyone who sees it. When people see it, their reaction is very noticeable. It’s like something they’ve never seen before. Finally! We can SEE my pain! I’m having an ultrasound Thursday. It’s like an edema, it looks like a big swollen bruise. It’s pretty large, the size of a dinner plate, and it’s where a lot, if not most, of my pain is! WTF? I’m calling this mystery blob of pain Nessy, for the Loch Ness Monster. It’s finally been photographed!
That might not look like much but keep your eye on the bump at the end of her finger.
excuse the shirt lines but you can see it above the shadow of the camera. Here’s another shot…
Above, the shark is pointing right to it. It’s my pain pillow! It hurts so much to lie prone on this blob. I didn’t even know it was visible until recently but I’ve felt it for years. The fact that it’s clearly visible, not just to me but to everyone, is huge. What could be producing such a big ugly edema?!
Hmmm, I wonder if it’s a lipoma? If it is, it could be coming from anywhere, I suspect close to my spine. If that thing goes below the surface it is definitely pressing on my spine and possibly my aorta. In some photos you can see it pushing onto the midline and the area next to the spine is the most painful spot on the blob. I’m glad that ultrasound is scheduled for tomorrow. We may have found it. This thing may have been growing for 12+ years.